First Aid in the Workplace
Right people, right kits, right procedures — accessible at every shift, on every floor, on every site.
- Run a first-aid risk assessment before deciding kit/first-aider numbers.
- Ratios: low-risk 1 per 50, high-risk 1 per 25, remote high-risk 1 per 10.
- CPR refresher annually, full requalification every 3 years.
- Kit: white cross on green, accessible, checked after use and at least every 12 months.
- Construction sites: identify first-aiders by distinct hi-vis colour and posted contact numbers.
1. Who's responsible
PCBU duties (WHS Reg 42)
- Ensure first-aid equipment is provided.
- Each worker has access at all times — including shift, overtime, night work.
- Provide access to facilities for administering first aid (clean area, ability to call 000).
- Adequate trained first-aiders, or workers have access to trained external first-aiders.
- May share equipment with other duty holders if adequate and easily accessible.
- Consult workers on kit location, contents, facilities and procedures.
- Cooperate with other duty holders on shared workplaces.
2. The first-aid risk assessment
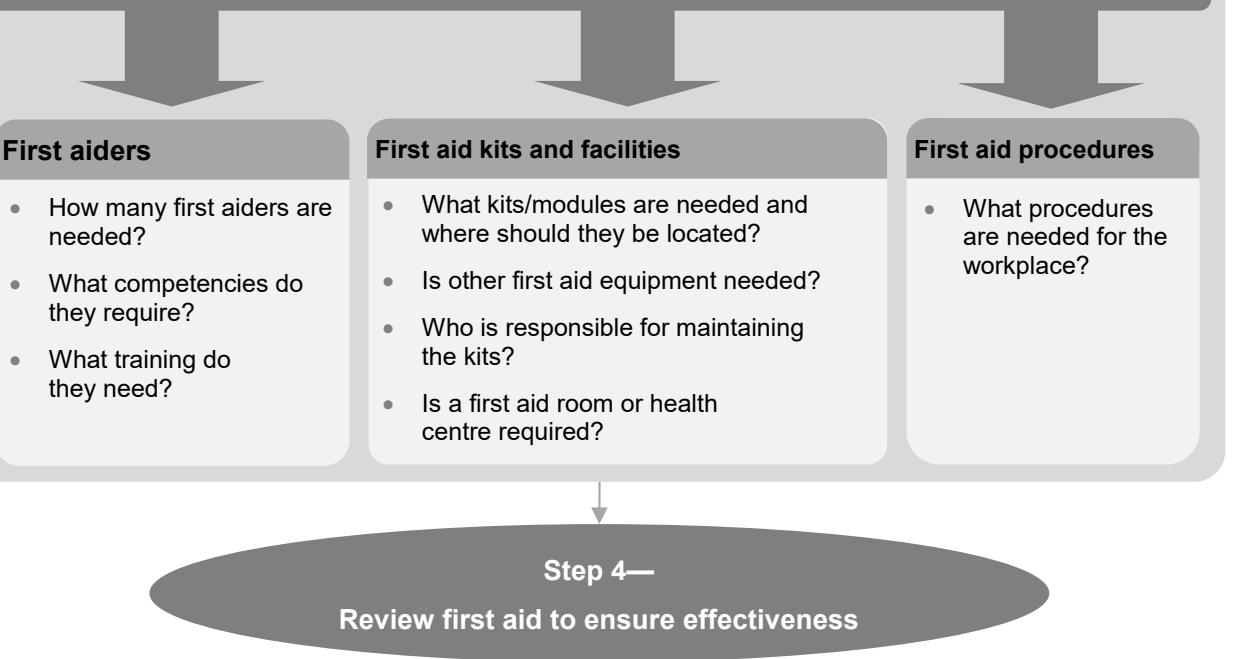 Figure 1 — First aid and the risk management process. Same 4-step loop, applied to emergency response capability.
Figure 1 — First aid and the risk management process. Same 4-step loop, applied to emergency response capability.
Consider:
- Nature of work and hazards — machinery, chemicals, electricity, heights, burns, biological, violence, animals, extreme temperatures.
- Workplace size and location — distances between areas, emergency-service response time, remoteness.
- Workforce composition — contractors, volunteers, visitors, workers with disabilities or known medical conditions (asthma, allergies, diabetes, cardiac).
- Injury likelihood data — incident history, near misses, SDS for chemicals on site.
- Emergency access — distance to hospital/medical centre. If timely access is unavailable, train to Provide Advanced First Aid (oxygen capable).
- Layout — multiple floors, dispersed workers, difficult-to-reach areas.
3. First-aiders — training & ratios
Minimum qualification: nationally recognised "Provide First Aid" Statement of Attainment from a Registered Training Organisation (HLTAID 009/010/011 unit family).
Recommended ratios
| Workplace risk | First-aiders |
|---|---|
| Low-risk | 1 per 50 workers |
| High-risk | 1 per 25 workers |
| Remote high-risk | 1 per 10 workers |
Currency
- CPR refresher: every 12 months.
- Full requalification: every 3 years.
Additional training where: remote/isolated work, dangerous substances (cyanide, arsenic, anhydrous ammonia), specialist equipment, children present, elevated psychological risk, workers with known pre-existing conditions.
Locating first-aiders on site
- Distinct hi-vis vest colour assigned to first-aiders only.
- Contact numbers posted prominently in multiple locations.
Coverage: train your own or arrange external first-aiders accessible during all shifts.
4. First-aid kits
Signage and design
 Figure 2 — Standard first-aid signage: white cross on green background.
Figure 2 — Standard first-aid signage: white cross on green background.
Kits must be: clearly identifiable, dust/moisture/contamination resistant, with contents list visible.
Minimum contents (typical workplace)
Gloves, gauze, saline, wound-cleaning wipes, adhesive dressings, tweezers, antiseptic spray, non-adherent pads (small/medium/large), conforming bandages (5 cm and 7.5 cm), 10 cm crepe bandage, scissors, adhesive tape, safety pins, wound dressings, triangular bandages, emergency rescue blanket, eye pads, instant ice packs, CPR face mask, instructions including CPR flow-chart, notebook and pen. Access to clean running water nearby.
Add-on modules
- High-risk (machinery, chemicals): extra eye pads, burns equipment, allergic-reaction equipment.
- Remote: heavy-duty crepe bandage, large clean sheeting, thermal blanket, whistle, torch.
- Outdoor: crepe bandage, sting-relief cream.
- Burn: hydrogel sachets, clean polythene sheets, burn instruction cards.
Location
- Prominent, accessible, near high-risk areas.
- One per floor in multi-storey workplaces.
- Portable kits in mobile workers' vehicles (couriers, taxis, sales reps).
Maintenance
- Nominated first-aider checks after each use and at least every 12 months.
- Replace used items immediately; verify expiry dates; sterile products sealed.
- Sign and date the inventory list.
No general medication
- Don't include paracetamol, aspirin, etc. — adverse-reaction risk.
- Asthma inhaler + spacer or epinephrine auto-injector only with appropriate training.
5. First-aid rooms
Required when: risk assessment shows administering first aid is otherwise difficult, or large/serious injury risk exists.
Recommended for:
- Low-risk workplace with ≥ 200 workers.
- High-risk workplace with ≥ 100 workers.
Contents: first-aid kit, hand cleanser, disposable towels, examination couch (waterproof, sheets), examination lamp with magnifier, cupboard, soiled-waste container, sharps disposal, ≥ 2 L bowl/bucket, power points, chair, table/desk, telephone or emergency-call system, first-aider and emergency contact details.
Location and features: near sink with hot/cold water; private (door or screen); doorway ≥ 1 m for stretcher access; well lit and ventilated; ~ 14 m² minimum; clearly signed.
Maintenance: assigned trained first-aider (unless a staffed health centre exists).
Health centres (large mines, remote sites): doctor/nurse/paramedic; ground-level if possible; self-contained; impervious easy-clean materials; quiet, away from hazards.
6. Special situations
| Situation | Key requirement |
|---|---|
| Remote / isolated workers | Aerial evacuation considered; effective communications; first-aider per 10 (high-risk). |
| Mobile workers | Portable kit in vehicle (secured against projectile risk); phone/comms to emergency services. |
| Lone workers | Documented emergency-response plan; comms; access to external first-aider. |
| Shift work / overtime | First-aiders accessible at every shift worked. |
| Public-facing venues | Consider visitors; AED may be warranted; possibly higher first-aider count. |
| Shared workplaces | Coordinate with other duty holders; sharing OK if adequate and accessible. |
7. Procedures
Written procedures should cover:
- Work areas/shifts; first-aiders' names and contacts.
- Types and locations of kits and facilities.
- Responsibility, inspection frequency, sign-off.
- Emergency communication (incl. remote/isolated worker protocols).
- First-aider training and worker induction on access to first aid.
- Worker health information: invite at induction (asthma, diabetes, allergies, cardiac) — kept confidential, shared only with consent.
- Injury/illness reporting chain.
- Blood and body-substance precautions: hand hygiene, PPE, sharps disposal.
- Post-incident transport and rest arrangements.
- Debriefing/counselling access for first-aiders and affected workers after a serious incident.
8. Records to keep
- Treatment register — record of treatments; reportable to management; subject to health-records law.
- First-aider training records — names, HLTAID unit, completion/renewal dates, CPR refresher dates.
- Kit maintenance log — signed/dated inventory checks.
- Emergency contact details — accessible locations.
- Worker health information — confidential, consent-based, for first-aiders only.
- Incident, injury, near-miss data — feeds into the next assessment review.
9. Construction-specific notes
- Multi-floor or dispersed sites: kit on each floor (or every second floor); central first-aid room with satellite kits.
- First-aiders identified by distinct hi-vis vest colour and posted contact numbers.
- Site induction includes how to call a first-aider, kit locations, evacuation routes.
- Sub-contractor first-aid arrangements covered in the WHS Management Plan under the 3C arrangements (whs_consultation_cooperation_coordination).
10. Common pitfalls / quick wins
Do
- Run the assessment before deciding kit and first-aider numbers — generic minimums don't suit every site.
- Consult workers on first-aid arrangements.
- Keep kits visible, accessible, prominently signed.
- Check kits after each use and at least every 12 months; date and sign.
- Ensure first-aiders are easy to locate (vest colour, posted contacts).
- Train extras for shift/overtime cover.
- Provide AED, eye-wash and emergency showers where reasonably practicable.
- Review first-aid every 1–3 years and after any change.
Don't
- Rely on a single first-aider for a large or dispersed site.
- Skip the assessment; cookie-cutter kits don't suit all hazards.
- Stock paracetamol/aspirin or other general medication.
- Neglect remote/isolated workers — confirm comms and external first-aid arrangements.
- Forget to debrief and offer counselling after a serious incident.
- Assume "shared" equipment is adequate — confirm accessibility with the other duty holder.
- Skip infection control (gloves, hand hygiene, sharps disposal) — every time.
11. Cross-references
- See also: risk_management_process, whs_consultation_cooperation_coordination, workplace_environment_and_facilities
- Glossary: glossary_and_key_concepts
- Construction site application: 02 - Construction Work/general_construction_work
Source: first_aid_code.md (Safe Work Australia, model Code of Practice, CC-BY-NC 4.0). Edition: July 2019. Last verified against SWA: 2026-04-27.